BACKGROUND
Acute diarrhea is the second most common cause of morbidity and mortality worldwide in under-five children.[1-3] Diarrhea is defined as an abnormal increase in daily stool fluidity, frequency, and volume from what is considered normal for an individual.[4-6] Diarrhea kills an estimated 2.5 million people each year, with about 60–70% of them being children under 5 years of age.[7-9] The disease is responsible for over a quarter of the deaths of children in the world today.[10,11] Most of these deaths occur in the developing countries where an estimated 25% of under-five mortality is directly attributed to diarrhea disease.[7,8,12] Oral rehydration salt is a balanced mixture of glucose and electrolytes, which if it dissolved in water the mixture is called oral rehydration solution (ORS).[13-15] ORS is used for treating and preventing dehydration, potassium depletion, and bicarbonate deficit due to diarrhea.[13-15] Despite the common use of oral rehydration therapy (ORT), the incidence of acute diarrheal diseases has not waned much, though a considerable decrease in the annual diarrheal deaths from 4.5 million in the 1980s to the present level of about 2 million children is ascribed to the promotion of ORT.
This is because most populations of the world, especially African countries, lack access to drinkable water and are still overwhelmed by poverty, lack of hygiene, and poor sanitation. Mothers, all over the world, especially in developing countries, have been taught the types, use, and importance of ORS. Furthermore, household sanitation, basic hygiene, and adequate appropriate feeding are underscored in different health clinics and well-child visits. Although these attempts have been shown to reduce the severity of acute diarrheal episodes and sharply decrease the number of subsequent death, a substantial number of children are still suffering from diarrhea that has an undesirable impact on their growth and development.[12,16-18]
This study aims to evaluate the knowledge, attitude, and practice of the use of ORS in the management of diarrheal disease among under-five children and also to make appropriate recommendations based on the findings.
METHODS
The study was conducted in Eguare, a rural community located in Irrua, Edo State, Nigeria, from May to September 2011. It was a cross-sectional study design. Respondents were mothers resident in the community with at least a child under the age of 5 years.
The study was carried out using the cluster sampling technique. As the community had seven quarters, four quarters were selected at random and all women of childbearing age with under-five children in the selected quarters were included in the study. The method of data collection was through interview-administered questionnaires.
Data were represented in table, charts and frequencies and analyzed using the IBM SPSS version 20.0. Test for statistical significance was performed using Chi-square at 95% confidence interval.
RESULTS
The result revealed 150 respondents, with mean age of 29.9 ± 6.8 years [Figure 1]. About 95.3% had knowledge about the causes of diarrhea [Figure 2], 72% had knowledge about the signs of dehydration [Figure 3], 98% were aware of ORS [Figure 4], but only 37.2% had used ORS when their children had diarrhea. Regarding the assessment of respondents’ primary treatment options for diarrhea, 32.7% commenced their children on ORS when they had diarrhea, 49.3% preferred to use drugs in the treatment of diarrhea, while 11.3% took their children to the hospital when they had diarrhea [Figure 5]. There was an association between the level of education and the practice of respondents in the treatment of diarrhea [Table 1]. (X2 = 18.498, P = 0.047)
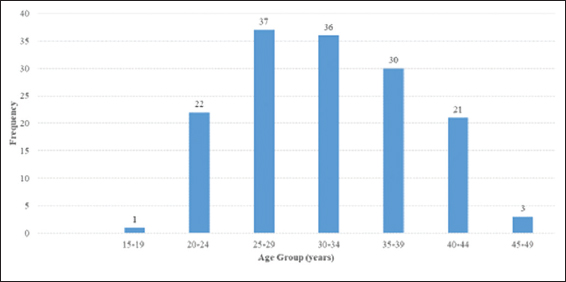
Figure 1: Age distribution of respondents (mean age = 29.9 ± 6.8)
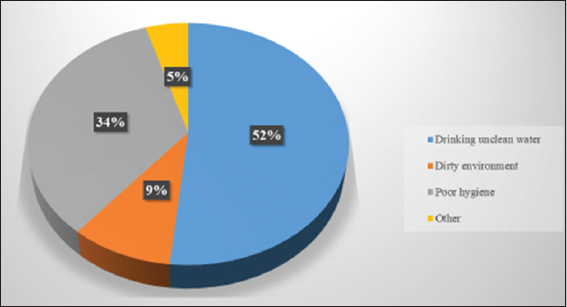
Figure 2: Respondents’ knowledge on the causes of diarrhea. About 77 (51%) respondents attributed diarrhea to drinking unclean water
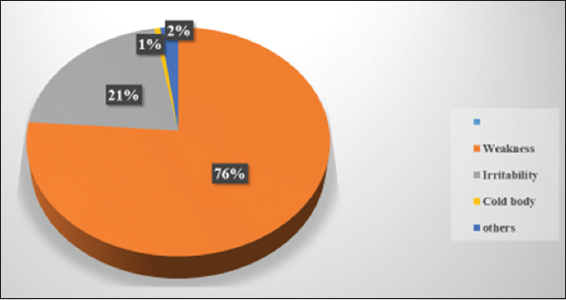
Figure 3: Respondents’ knowledge on the signs of dehydration. 109 (76%) respondents notice weakness as a sign of dehydration when their children have diarrhea
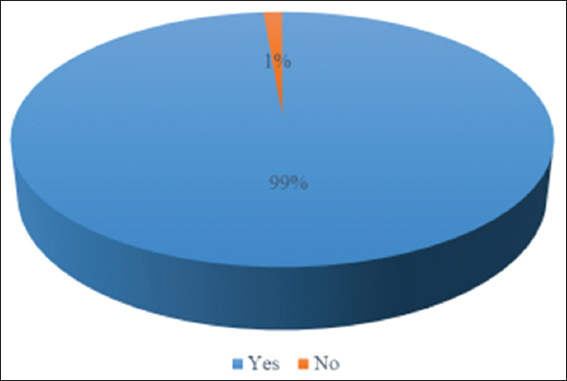
Figure 4: Mothers’ awareness of oral rehydration solution (ORS). 148 (99%) of respondents are aware of ORS
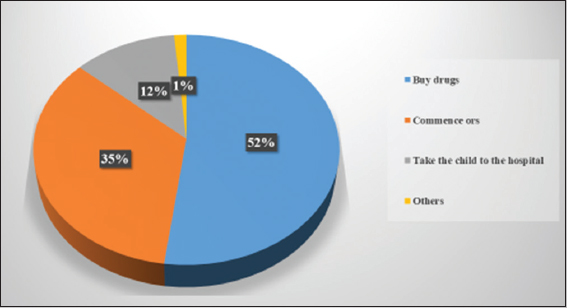
Figure 5: Respondents’ practice of diarrhea treatment. About 50% respondents use drugs as the primary treatment option for diarrhea
Table 1: Association between level of education and respondents’ practice of diarrhea treatment

DISCUSSION
This study assessed the knowledge, attitude, and practice of mothers the use of ORS in the management of diarrhea in under-five children. The results revealed that 95% of respondents had knowledge on the causes of diarrhea [Figure 2] which is similar to a study done by Agbolade et al., 2015, in Ibadan, Nigeria, which showed that 88% of respondents had knowledge on the causes of diarrhea.[19]
In this study, 98% were aware of ORS [Figure 4], but only 37.2% used ORS when their children had diarrhea. In a similar study done by Agbolade et al., 2015, in Ibadan, Nigeria, 98% were aware of ORS, but only 49.5% used ORS when their children had diarrhea.[19] Similar study conducted by Ogunrinde et al., 2012, in Zaria, Nigeria, showed that ORS use was abysmally low at 8.6%.[20]
Regarding the assessment of respondents’ primary treatment options for diarrhea, 32.7% commenced their children on ORS when they had diarrhea, 49.3% preferred to use drugs in the treatment of diarrhea, while 11.3% took their children to the hospital when they had diarrhea [Figure 3]. A similar study conducted by Agbolade et al., 2015, in Ibadan, Nigeria, showed less use of drugs: Orthodox (22.6%) and native medicine (3.7%) in management of diarrhea with 72.7% taking their children to the hospital when they had diarrhea.[19] Ogunrinde et al., 2012, in Zaria, Nigeria, reported that the use of antibiotics and antidiarrheal agents constituted the first line of action in 36.1% of caregivers with only 8.6% employing ORS in the treatment of diarrhea, while a further 45.7% took their children to the hospital when they had diarrhea.[20]
CONCLUSION
There is a need for health education of women, especially in the rural community, in the use of ORS in the prevention and treatment of dehydration due to diarrhea and also to discourage self-medication practices in the management of diarrhea.